
by Gil Poulsen | Oct 21, 2015 | Mac, Medical, Technology
THAT’S MY PET NAME for the newly-arrived Mac OS X 10.11 (aka “El Capitan”), given how one is virtually bludgeoned into upgrading with incessant App Store notifications. Even as cautious an early adopter as I took the plunge the day 10.11 was released, but only because 1) I was curious to test Apple’s assessment of this upgrade being a straightforward “tune-up” and unlikely to cause any serious heartache for those choosing to live on the bleeding edge of Mac OSs, and 2) I was fully Time-Machined in the event of disaster.
To my surprise, life after Yosemite has been markedly uneventful, to the point where I’ve had to set my desktop to the default El Capitan image to remind me that I’m no longer working in Yosemite. Then again, the new features are so underwhelming this time around that your everyday computing experience will be little changed; the most compelling new feature could be the ability to locate a “lost” cursor by shaking your mouse to temporarily enlarge the pointer. Seriously.
Yes, the Notes app has been upgraded with to-do lists and the ability to attach an image or link, and Safari now has pinned tabs, although its implementation is somewhat flawed when compared to the Chrome browser, which has had this feature for ages (in computer terms, anyway). Beyond that, toss in some increased performance and stability, a few Spotlight improvements and the ability to sort albums in Photos by something other than the title of the image, and that pretty much covers it.
NOW WE KNOW why Apple kept virtually mum about El Capitan at their September 9 event. Fact is, I had planned on devoting a lot of keystrokes to the OS X 10.11 experience, but I think that about covers it. Other than, of course, whether you should take the plunge yourself at this point.
Here’s my advice, for what it’s worth. If you have not already done so, wait for OS X 10.11.1, which should be arriving in a month or so. That will give Microsoft and Apple time to work out the Office 2011/2016 crashing issues, in particular with the Outlook mail app (which hopefully none of you are forced to use), and address the most egregious bugs that a few users have reported.
Now, on to more compelling stuff:
Only a few feathers short (for now)

There’s no danger anyone’s going to make a verb out of using it (“just DuckDuckGo it”?), but even Google might be more than a little concerned about the upstart search engine DuckDuckGo, The Search Engine That Doesn’t Track You, as its landing page proclaims proudly.
Right from the get-go, DDG was on a mission to not profile its users, and prides itself on not altering its search results based on what it knows about the searcher, practices in which Google has been actively engaged since at least 2009.
DuckDuckGo uses data from Wikipedia and from other search engines like Yahoo! and Bing (with their consent), so it’s not as thorough or accurate as Google, and lacks some of the higher-end features like the search giant’s Knowledge Graph, currency conversions and other calculations, flight info, etc. It can, however, perform a few nifty tricks that Google can’t.
But the real lure of DDG is that it provides uniform results to all; in fact, that’s all it can do because it doesn’t track your browsing history, and therefore has nothing to go on when it comes to custom-tailoring your search results. Should you find yourself so inclined to Google “how can I stop Google from tracking me on the web,” you’ll notice more than a few references to DuckDuckGo.
Thanks to its emphasis on personal privacy, DDG suddenly found itself on a relatively level playing field last year when Apple added DuckDuckGo to Safari (and Mobile Safari) as an optional search engine in September 2014. Mozilla (Firefox) followed suit soon after. Tip: Don’t hold your breath waiting for the Google Chrome browser to add DDG (although a Chrome extension for DuckDuckGo does exist).
Is it worth taking a flyer on this upstart search site? I’ll let you folks decide. On your Mac, go to Safari–>Preferences–>Search to set DuckDuckGo as the default search engine; for your iDevice(s) it’s Settings–>Safari–>Search Engine. Who knows? Maybe you’ll find that Google just isn’t all it’s quacked up to be, and should that be the case, DuckDuckGo might just… fit the bill.
More, more, more

DID ANDREA TRUE’S 1976 disco classic predict Apple’s own October surprise of last week, what with the wizards of Cupertino announcing more, more, more new gizmos only a month after September’s iPhones, iPads, Pencils and Smart Keyboard?
OK, probably not, although given that the history of this tune involves a porn actress, former Jamaican prime minister (and Castro sympathizer) Michael Manley, and a 2011 Honey Bunches of Oats commercial, I couldn’t resist conjuring one of my usual tortured references here. But honestly, I suspect “more, more, more” most appropriately describes the amount of cash you’ll need to get your hands on any of these gadgets:
| Peripheral | Magic Mouse–>
Magic Mouse 2 | Wireless Keyboard–>
Magic Keyboard | Magic Trackpad–>
Magic Trackpad 2 |
| Was | $69 | $69 | $69 |
| Now | $79 | $99 | $129 |
| Which is… | More, | More, | More… |
The Magic Trackpad has Apple’s new Force Touch and a larger surface area, the Magic Mouse 2 is lighter with fewer moving parts, and the Magic Keyboard is… well, it’s the Magic Keyboard and not the Magic Keyboard 2, because the previous model was technically known as the Apple Wireless Keyboard, as opposed to the Magic Keyboard. This new one has, uh, keys and a spacebar and stuff. And now, it’s officially magic.
These pricey new peripherals finally(!) do away with the need to keep a stockpile of AAs at the ready, since all three use lithium-ion batteries that reportedly charge fully in just a few hours via a Lightning to USB cable (included), while squeezing about a month of average use from a single charge.
Before you decide to experience all this magic for yourself, you should know all three of these doodads require you to be running the brand spanking new OS X 10.11 El Capitan operating system on your Mac of choice. Furthermore, that Mac must be Bluetooth 4.0 capable (meaning 2012 or newer models, give or take a few months).
What’s that, you say? You’re saddled with the virtually prehistoric “mid-2011” iMac? Or perhaps an Industrial Revolution-era “late 2011” MacBook Pro? No worries, Apple’s got your back with—what else—more iMacs, with more pixels, for more money! The new 21.5” 4K “Retina” iMac, at $1499 ($400 more than the previous model) has four times more pixels (~9.4 million; 4096 x 2304) than its $1099 cousin (a paltry 2 million or so).
Still not enough pixels for you? The $1799 27” 5K iMac’s display offers a staggering 14.7 million pixels (5120 x 2880), which, at a mere $0.0012 per pixel, just might qualify as the bargain of the century. To say nothing of the fact that you get a “free” Magic Mouse 2, Magic Keyboard and Lightning to USB charging cable in the box!
Need I say more… more… more?
The password is… not?
AND NOW, HERE’S some wonderful news for those of us whose “things I really, really hate a lot” lists read something like this:
Things I Really, Really Hate A Lot
- Passwords
- Stuff that needs passwords
- Password managers
- Password managers that need passwords
- The 1-877-KARS-4-KIDS jingle
- Squirrels
- Anything that seems even vaguely French
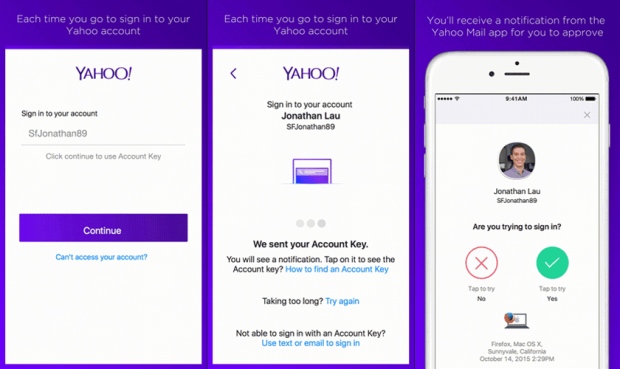
Assuming your #1-#4 are similar if not identical to mine, Yahoo! is coming to your rescue here, with a radical new authentication option for Yahoo! Mail they call Yahoo! Account Key. I’ll spare you the technological mumbo-jumbo about two-factor authentication and get right down to the nitty gritty: Account Key enables you to log into your Yahoo! email in a Web browser just by receiving a notification on your mobile phone and touching “OK.” No fuss, no muss—and no password!
Is it secure? Yes. Is it easy to set up? Yes. Does it work for anything else besides Yahoo? No. Not yet, anyway. But the hope is that others (Apple, Google, etc.) will soon follow suit. The predecessor of Yahoo Account Key, the aforementioned two-factor authentication (2FA), requires that you enter a password and a temporary PIN code, typically supplied by a notification or SMS (text) message on your cellphone.
YOU CAN USE 2FA right now with your Apple ID, Gmail and a host of other services, but most of us would prefer to make it easier to access our online properties, as opposed to harder—even if setting up and using 2FA does make things quite a bit more secure than passwords alone. And if you don’t have a mobile phone, well, then it’s time to start learning the ins and outs of your password manager of choice.
For more info, check out Glenn Fleishman’s take on Yahoo Account Key at Macworld.com, as well as the official announcement from Yahoo.
October surprise
NO, I’M NOT REFERRING to that kind of October surprise; we’ll have to wait a year or so to see what may be lying in wait—and for whom—in the weeks leading up to the 2016 presidential election. I’m talking about a very gratifying surprise for me personally, which just happened to occur on October 10 when I completed a 60-mile bike ride from Piscataway to Ortley Beach with relative ease, and with no ill effects.
I’d done this annual “Tour de Shore” ride at least a dozen times since the 1990s, but was forced to place myself firmly within the “maybe next year” category ever since a July surprise of 2011, when a routine blood test showed I had virtually no platelets. That was followed by a diagnosis of acute myeloblastic leukemia one year later, and finally by a Halloween 2012 stem cell transplant.
Due to the aftereffects of the chemo regimens, and the chronic graft vs. host issues that followed the transplant, I had become pretty much resigned to the idea that I should feel blessed merely to be able to make it from the bedroom to the living room without passing out, and set aside even the slightest notion whatsoever of engaging in any long-distance cycling activity.
BUT MODERN MEDICINE seems to have no shortage of miracles these days, and I’m happy to report that since then my overall health and vigor have gradually returned, particularly over the past year, defying my own assumptions that I’d “plateau” at the point where I could perhaps manage a walk around the block, but little more. Cycling, on the other hand, would be an activity heretofore banished to the “things I used to do before the transplant” category.
That’s why completing this year’s ride really did come as a surprise to me, especially given that I truly was not physically capable of completing it only a year ago. This time around, in spite of being a full year older, I felt I could have endured even a few more miles at the end of the ride.
What’s also been surprising to me—though it probably shouldn’t be—is the degree of support and good wishes I’ve received from so many of you since this whole ordeal began. So thanks again to family, friends and all of you out there for your positive thoughts and your encouragement along the way.
It’s been quite a ride.
by Gil Poulsen | Dec 16, 2014 | Mac, Medical, Technology
While hard at work on an AltiM@c holiday greeting for your reading (and perhaps even singing) pleasure, it struck me that there are more than a few Mac-specific concerns deserving of at least some mention here, before we find ourselves ringing in the New Year.
So without further ado, here’s a quick Q&A focusing on the issues many of you have been encountering as of late:
Q. Is it finally safe to upgrade to Yosemite?
A. That’s a qualified “yes.” Now that Apple has released the 10.10.1 bug fix, I can’t find any compelling argument against making the jump to Yosemite. My only note of caution would be that those of you still using OS X 10.5 (Leopard) or 10.6 (Snow Leopard) with pre-2008 versions of some programs (Office 2004, Adobe Creative Suite 2 or earlier, Quicken 2007 to name a few) will need to buy some newer software. Hey, at least Yosemite itself is free…
Q. What about iOS 8?
A. Now that they’ve put the Camera Roll back, and the iCloud Photo Library seems to be working quite well, I absolutely think you should move up to iOS 8. Users of the iPad 2 and the iPhone 4s who are concerned about performance with the newest iOS have little to fear, since the iOS 8.x bug fixes rectified those issues for the vast majority of users. Then again, if you’re using an iPhone 4s you’re way overdue for an upgrade anyway. Speaking of which…
Q. Should I get the iPhone 6/6+?
A. I’m kinda mixed on this. Yes, they are both awesome in terms of speed, display quality and camera, and the iPhone 6+ screen is massive in comparison to its forebears. My concern with the 6+ is that it’s just too big to handle comfortably in one hand, and presents a challenge to those who spend some part of their day inserting and removing their phone from their front pants pocket. Even the 6 is on the tall side…
My advice would be to get the 5s while it’s still available and $100 less, since the only really significant feature missing from the 5s versus the 6 is the ability to use Apple Pay. But hey, if you really want/need a larger screen and you don’t keep your phone in your pants pocket, don’t let me talk you out of a pretty remarkable piece of hardware.
Q. Why do I keep getting “blocked plug-in” messages?
A. You can thank the Adobe Flash plug-in for that, as well as all the Web site developers who still insist on using Flash for video and other content on their sites. Given that the iPhone and iPad, as well as the vast majority of Android tablets, seem to get along just fine even though they can’t even run Flash, I eagerly await the day when Flash no longer exists on any platform.
But until that glorious day arrives, you’ll have to keep checking your System Preferences–>Flash Player settings to ensure you have the latest version. In some cases Flash will update itself without troubling you with error messages, but when there is a significant update to the plug-in, you will need to manually install it in order to banish those infernal “blocked plug-in” messages. At least, until the next update.
Here’s some helpful guidance on keeping Flash up to date, courtesy of Adobe. Hey, it’s the least they can do.
http://helpx.adobe.com/flash-player.html
Q. What’s the deal with those special eyedrops you were getting?
A. Oh, thanks for asking. I’ve been using them for a few weeks now and I can’t really say that I have seen any significant improvement, but since everyone’s immune system is unique (not many more so than mine) my immuno-ophthalmologist really couldn’t tell me exactly what to expect in terms of efficacy or a time frame. So we’ll, uh, see…
Q. Can I ask one more “computer” question?
A. Sure.
Q. Thanks. I know I should be backing up my iDevice, but should I back it up to my Mac or to iCloud?
A. Definitely to your Mac (or Windows PC, if that’s how you roll). Why? Storage on your computer is free, as opposed to your having to pay for additional room on iCloud for all those fab pix and videos you have on your iDevice(s). And the local iTunes backup is more complete than the iCloud backup.
But… if you can’t be troubled to plug your device into the computer once a week or so, and/or you’ve already ponied up for extra iCloud storage, then iCloud is just fine. What’s important here is that you are backing up your iDevice(s) somewhere.
Q. OK, I think that’s it for now.
A. No problem, give a shout if you have any other questions.
by Gil Poulsen | Oct 31, 2014 | Medical
APOLOGIES FOR the lurid yet fiendishly-clever-as-usual title, but trust me–it’s no less appropriate than was last week’s POODLEs reference. Not only is today All Hallows’ Eve, a time for all things sanguinary, but it just happens to be the 2nd anniversary of my stem cell transplant, undergone whilst witnessing the devastation of Hurricane Sandy from my hospital room window.
Plus, I’m way overdue for a medical update, and what with all the security breaches and new operating systems with which we’ve been inundated recently, I figured you could use a break from the geeky computer stuff. So let’s jump right into some geeky medical stuff instead.
As I noted right around this time last year, the sheer volume of blood moved in and out of one’s body prior to said transplant is about as sanguinary as it gets. Yet through it all, the docs and I remained sanguine and thus, here I prattle to report on my current condition re: chronic graft vs host disease and an innovative but, ah, sanguinary new treatment for that most vexing of conditions afflicting much of the cGVHD population–keratitis sicca, a.k.a. dry eye.
BECAUSE OF the way cGVHD causes a stubborn and severe inflammation of the tear ducts, we transplant patients end up with a pretty high-octane version of dry eye–the kind that is virtually debilitating at times, and doesn’t respond to artificial tears, lubricants or even the vaunted Restasis–although that does seem to work quite well for the attractive eye doctor in the TV commercial.
So what have the best and brightest researchers recently conjured for us keratitis sickies? As you’ve probably deduced from all of the above, it has everything to do with… blood.
Seems that the only area of our body that is not threaded through and through with blood vessels is the cornea–the clear outer covering of the eye over the pupil. Clear being the operative term here–if the cornea were intertwined with blood vessels, it would no longer be clear, and we’d have only four senses with which to work.
SO HOW DOES the cornea receive the nutrients that blood transports to all the rest of our cells, if the blood has no way to get there? Why, tears of course. Seems they’re not just for keeping your eyes lubricated (courtesy of the tear film that covers and protects the cornea); they also carry the same nutrients that your blood supplies to all other parts of your body.
These researchers therefore theorized that if they mingled the blood from an individual suffering from severe dry eye with artificial tears, in just the perfect proportion, they could create an autologous serum in the form of eye drops that would work as well as the real McCoy. Tears of renown, if you will.
Sounds simple, perhaps, but the early returns have been promising. Here’s an excerpt from a recent study published at the Wiley Online Library:
Theoretically, autologous serum eye drops (AS) have a potential advantage over traditional therapies based on the assumption that AS serve not only as a lacrimal substitute to provide lubrication, but also contain other biochemical components mimicking natural tears more closely. The application of AS in dry eye treatment has gained popularity as a second-line therapy in the treatment of dry eye. Published studies on the subject indicate that autologous serum could be an effective treatment for dry eye.
THE REST, as they say, is history. To wit: In a most happy coincidence, AS happened to be exactly what Manuel B. Datiles, M.D., the ophthalmologist with whom I was fortunate enough to meet at last year’s NIH trial, was–and still is–experimenting with.
This smidgen of information I gleaned at the trial led me to broach the subject of AS with one Leonard Bielory, M.D., he of the STARx Allergy & Asthma Center in Springfield, NJ and the immuno-ophthalmologist I’ve been visiting recently. In an even happier coincidence, he’s already been preparing AS for some of his patients, and has offered to whip up a batch for yours truly in the very near future–but only if I agree to just a little more bloodletting, of course.
TO WHICH I say: Why not? It is Halloween, after all. And what’s Halloween without a little, er… blood let for tears.

The Team G pumpkin, as carved by sister Lori and family
Next: Back to computer/technology stuff that I’ll pretend you’re actually interested in
by Gil Poulsen | Mar 26, 2014 | General, Medical
In the aftermath of Hurricane Sandy, the Long Branch Arts Council announced in February that they were seeking submissions from New Jersey poets of all ages to write about their personal experiences or impressions focusing on the events of this “superstorm” and its aftermath. Those submissions will become part of an anthology entitled “Poetic Voices In Response To Hurricane Sandy.”
Since I’ve had what I consider to be a somewhat unique “Sandy” experience, I figured I’d submit my story to them, and also share it here with you. Plus, all that writing won’t go to waste should the powers that be at the Arts Council decide that my submission is not up to their standards…
THE KENNEDY ASSASSINATION (1963) is a prime example, although you’d probably have to be pushing 60 to have a specific recollection of that one. For those like me, who’ve been around for only a half-century or so, the Challenger space shuttle disaster (1986) certainly qualifies, as does the death of John Lennon (1980) and most recently, the terrorist attacks of September 11, 2001.
Over the course of anyone’s lifetime there are events such as these, events of such significance that it becomes possible to recall precisely where you were and what you were doing at that very instant.
Psychologists call these vivid recollections “flashbulb memories” because, like a camera’s flashbulb going off, they briefly illuminate and capture a moment that is typically both surprising and consequential. These unique recollections can be extremely detailed, highly accurate, and also very difficult to forget.
For me—and doubtless for all residents of the Jersey Shore—it’s hard to imagine anything more difficult to forget than Superstorm Sandy. Due to circumstances unique and somewhat beyond my control, I’ve managed to amass an entire album of these flashbulb memories from the events of that time—in spite of the fact that those recollections have little to do with the storm itself, or with its aftermath.
Then again, you might say they have everything to do with it.
ON OCTOBER 29, 2012, as Sandy made landfall along the southern N.J. coast, I was not doing what every other Bradley Beach resident—including my wife Donna and our two cats—had been advised to do, which was to grab some valuables and a change of clothes and head for higher ground.
I’d like to say that this was due simply to a can-do spirit and a steely determination on my part to damn the torpedoes and ride out the storm—sans heat, electricity and high-speed Internet. But that’s as far from the truth as I was from our condo at the time, so the decision to stay or to go was out of my hands.
What is true is that pretty much everything else was out of my hands as well, and on that morning I was an hour or so away from the Jersey shore, having spent the last few months riding out a storm of an entirely different nature, and preparing anxiously for the worst it had to offer.
Specifically, I was staring out the window of the bone marrow transplant unit of New Brunswick, N.J.’s Robert Wood Johnson University Hospital, awaiting the arrival of a shipment of HLA-matched stem cells provided by a most gracious, generous and compatible donor from the state of California. I had been diagnosed with an acute myeloblastic leukemia earlier that year, a type of cancer that can be temporarily controlled but not cured via the multiple rounds of chemotherapy I had undergone over the summer.
So for me, a transplant of stem cells from a compatible donor was the only option for long-term survival. My doctors, having determined this even prior to my first admission and chemotherapy treatments that July, had already begun a donor search. My two sisters were unfortunately ruled out early on, much to our collective disappointment.
EVENTUALLY TWO POTENTIAL DONORS were identified; the first disqualified due to an incompatibility in blood makeup but the second found to be fully compatible. Once this donor had been cleared, I immediately underwent further chemotherapy in order to obliterate every trace of my own bone marrow, along with the majority of my immune system.
This process, known as myeloablation, would allow the donor’s stem cells to be transplanted into my body without being rejected as they otherwise would have been. If the transplant “took” successfully, the donor’s stem cells would create new hematopoeic (blood-producing) and cancer-free bone marrow, as well as an entirely new immune system to replace what was left of my own.
As with so many things in life, timing is everything. The myeloablative chemotherapy I underwent in preparation for the transplant left me not only without a functioning immune system, but also without the ability to generate blood on my own. I’ll leave it to your imagination to ponder the long-term prospects for an individual allowed to remain in such a state, but suffice to say there is a fairly narrow window within which to initiate the transplant; i.e. the donor’s stem cells, which have a relatively brief “shelf life,” need to arrive on schedule before they—or the recipient—expire.
Yet for transplants like these, the timing is typically not an area of great concern, given that a cross-country flight can be accomplished in the space of an afternoon and that stem cells intended specifically for transplant remain viable for a period of at least a few days. But let us consult our flashbulb memories of that time and recollect that at that very moment the entire East Coast was being hammered by a “superstorm” and that power was out for millions, airports were closed to arriving and departing flights, and gas stations were either shut down or open but without any gas to pump.
Given that, it doesn’t take a Ph.D. (with all due respect to the brilliant and capable Roger Strair, M.D. and Ph.D.—and my oncologist at RWJ) to realize that it was going to require nothing less than a Herculean effort to deliver anything—much less a package of living human cells with a relatively brief expiration date—from southern California to New Brunswick, N.J. under those conditions.
WHICH BRINGS US back to the morning of October 29, 2012. From my perspective, there were actually two storms wreaking havoc—one outside the window of my hospital room, and one inside of, well, me. As the hospital was fully equipped to weather an external storm of even Sandy’s magnitude, their generators had kicked in within minutes of the first power outage, and I found myself lacking little in creature comforts compared to the millions around me without heat, hot water, electricity, gasoline—or in some cases, even a place to live. For me, experiencing the effects of Sandy was akin to watching a documentary on the event—the chaos wrought by the storm all passed quietly outside my window as if on a movie screen, with little effect on my daily routine.
At the same time, however, I—and I assumed the hospital personnel as well—were at least somewhat concerned about the prospects for a timely delivery of my prospective stem cells to the bone marrow transplant unit. As was my wife, who, being the more pragmatic member of our family, had already concluded in my absence that a friend’s offer of temporary housing in their conveniently-untenanted apartment in Middlesex County was without question the most sensible option for her and for our cats, a decision with which I agreed wholeheartedly.
Although the apartment complex was subject to the same power outage affecting the area around the hospital, it was quiet, safe, and at least somewhat warmer and drier than most of the homes on the Bradley Beach oceanfront. One crisis averted, but as Sandy’s impact on the local infrastructure continued to worsen over the next few days, I grew more apprehensive about the timely arrival of the stem cells. If the nurses and specialists with whom I had daily contact were equally as concerned, however, they did little to betray those feelings and were quick to reassure me that they would indeed arrive, if not precisely on schedule, at least within the window of opportunity for a successful transplant.
Which they eventually did, via a re-routing of the aircraft carrying the shipment to Buffalo, N.Y.—the nearest airport open for business—followed by the odyssey of an extremely dedicated and resourceful courier who managed to deliver the cells from upstate New York to the hospital a mere one day behind schedule, in spite of closed roads, downed trees, non-functioning traffic lights and a limited selection of gas stations along the way. The transplant, delayed by exactly one and one half days, took place on Halloween—perhaps a fitting coincidence given the amount of bloodletting involved on both my and my donor’s parts in preparation for my eventual resurrection.
WHILE SANDY REMAINS the common thread uniting our collective recollections of late 2012, I feel reasonably confident in stating that my own “flashbulb memories” of that time—when contrasted with the majority of Jersey shore residents—are as different as they could possibly be.
And precisely the same.
by Gil Poulsen | Feb 5, 2014 | Mac, Medical, Technology
I’ve been accumulating a bunch of Mac-specific topics about which to blog, none of which seemed to merit an entire posting. So I’ll devote a paragraph or two to each here, and even toss in the latest on my post-transplant cGVHD status, since I’ve always believed that a blog post without mention of hemoglobin levels or corticosteroid tapers hardly merits your valuable time or attention.
Remote excess
FYI for those of you with whom I engage in periodic remote support sessions: I’ve transitioned completely now from the Schnitz Remote Lite app, my former remote assistance tool of choice, to the TeamViewer Quick Support app. So… if you still have Schnitz in your Applications folder or in your Dock, you can trash it, and if you don’t yet have the TeamViewer Quick Support app, you can download it from my “cloud” here:
http://media.altimac.com/TeamViewerQS9.dmg
In fact, even if you do have it, those of you who haven’t used it within the last few months should download this one and replace your current one, since this is a more recent version.
Maver-icky?
By now most of you have been prompted via Apple’s Software Update to download and install “Mavericks” (aka Mac OS X 10.9). If you haven’t already done so, my advice is to continue to hold off for a bit. My experience to date has been that the issues resulting from the update, particularly with the Apple Mail program and with user directory and file permissions make it not worth doing at this point. The new feature set overall is arguably useful yet pretty underwhelming (a dedicated Maps app like on the iPhone, a tabbed Finder, tags for documents) so I’d have to say the pain is not worth the gain–yet. Figure on maybe dipping your toe in the water when Apple releases the 10.9.4 version; they are currently about to release 10.9.2, so we’re talking somewhere in the late spring or so in terms of a timeframe for when it would be reasonably safe to upgrade.
Pro no, you don’t
While we’re on the subject of Apple stuff to avoid, I’ve got to put the new Mac Pro into that category. Not that there’s anything really wrong with it, it’s just that it’s so danged expensive even in its base configuration, which offers a mere 256GB of storage (even iMacs start you off with a full terabyte [1000GB]). That means you’re already into another grand or two to step up to a roomier option. Granted, the 256GB solid-state drive that comes in the Pro is wicked fast, but that speed doesn’t help you too much if you’ve already got 400GB of stuff on your current Mac. The Pro is a speed demon, it’s quiet, it’s portable (unlike the previous Pro models which one can barely lift), it’s got stunningly good looks, six Thunderbolt ports and Turbo Boost, but still… given the ~$5,500 price tag for a model with adequate storage, I’d rather get me, oh, two iMacs and a Mac mini and still have some cash to spare.
Taking my shots
Dropped in on RWJ/CINJ last Tuesday for the usual (blood work, a parking nightmare and still more immunizations) and my numbers were pretty much OK; my hemoglobin has remained in the 14.x range, ensuring that I have the requisite get up and go to create further blog postings and show up at your door when circumstances require a personal visit. I got three more of the seven vaccines I got last month, and need to undergo the remaining four again next week. And again in four months, yeesh. As far as the steroid regimen goes, my docs do want me to continue the taper but at the rate of only 10mg each month. So I’m not exactly thrilled about the pace, as it means it will be sometime this summer before I am tapered off completely ;-( Better late than never, of course…
Going (anti)viral
As irresponsible as it may seem–especially given that I’ve been voluntarily undergoing the battery of inoculations noted above–I still can’t comfortably recommend installing anti-virus software on a Mac. If you’re using Mac OS X 10.6 “Snow Leopard” or newer, the operating system automatically updates itself to deal with the most recent and severe threats, and more often than not, third-party antivirus utilities seem to cause more problems than they prevent.
CNET just reported on an evaluation of the most popular AV programs on the Mac side conducted by security researcher and analyst Thomas Reed, which found that neither the McAfee nor the Symantec products made it into the “top tier” of antivirus options for the Mac. ClamXav, which is open source and has a minimal footprint in terms of intrusiveness and performance issues, was not one of the best options either. ClamXav has heretofore been my “go-to” recommendation to anyone who feels compelled to install some form of protection on their Mac, so I may have to rethink my position on that one ;-(
The CNET article pretty much mirrors my own position, for what it’s worth, on AV software:
“Whether or not antivirus tools are recommended for OS X is a question that is still in a bit of flux. Hard-core Mac users often claim malware scanners offer more potential harm than good, especially given the relative lack of malware for OS X. However, this mentality butts heads with those who may not trust, or have, the abilities to avoid all potential avenues of attack on their systems.”
Tweet, tweet
It’s been a long time coming, but I’ve finally arrived at the conclusion that it might not be a complete and utter waste of time on my part to create a Twitter username, and perhaps even toss out an occasional tweet here and there. In spite of being an incredible time-suck, and disregarding the volume of mean-spirited and even hurtful tweets that are posted on an hourly basis, Twitter does indeed have some redeeming qualities–if you are discriminating in terms of which Twitterers you elect to follow.
I am neither suggesting nor recommending that you run out and create a Twitter account just to receive an occasional Mac-related tidbit from yours truly, but I’d like to get your feedback on whether you would find tweets from me interesting and/or useful enough to contemplate joining the Twitterverse. If you happen to be in the “I’ve always been curious about Twitter but don’t really understand it and have no clue as to how to get started” camp, I’ll be more than happy to dedicate my next blog post to that very subject.
Never fear–no matter how my position on social media sites may evolve, I’m still not joining Facebook.
Note: In the event this is not painfully obvious, you can follow anyone on Twitter without creating an account just by visiting their profile page. Example: Chicago Sun-Times technology columnist and Internationally Beloved Industry Figure™ Andy Ihnatko, or my favorite 320-lb, ex-N.Y. Giant and current North Kentucky River Monsters starting QB Jared Lorenzen, aka The Pillsbury Throwboy/The Round Mound of Touchdown/J. Load/<insert appropriate weight-related nickname here>.
by Gil Poulsen | Dec 23, 2013 | Medical
By now, it should be apparent that no genre of music–classic, holiday or otherwise–is immune from parody once I take keyboard in hand. This one’s a bit of a stretch, though, so stick with me here. When last I shared the most recent details of my multiple medical misfortunes, I had just returned from the NIH clinical trial in Bethesda and was preparing for a battery of childhood immunizations to replace those erased courtesy of the transplant process.
I’m happy to report that those seven shots did cover most of the old standards like hepatitis B, polio, diptheria, tetanus and pertussis, and therefore I should be able to go about my business confidently in the coming years, secure in the knowledge that no matter where my travels take me, I am protected from whooping cough and lockjaw.
I did find the measles/mumps/rubella vaccine conspicuous by its absence, but as it turns out I will need to get booster versions of all the aforementioned vaccines at the end of January, and yet again in November 2014, at which time they will apparently toss in the MMR vaccine as well. Those of you with young children have no doubt run this gauntlet in the recent past, but given how long its been since I was classified as an infant, it just seems like a heckuva lot of needles in a very short period of time.
I’ll now dispense with my trypanophobic whinings and move on to the part where I try to make some sense out of this posting’s title. I have not touched on the subject of corticosteroids in some time, so why not take this opportunity to somehow employ them to pervert one of our most treasured holiday carols? As most of you are aware from my earlier missives, the only practical and effective way to restrain and control the symptoms of chronic graft vs. host disease (cGVHD) is to administer a whopping dose of prednisone, and then hope that the symptoms don’t return once the dose is tapered off.
Since prednisone is not a cure for cGVHD, it comes down to a “cross your fingers” scenario that said symptoms remain at bay; otherwise one must immediately revert to the original dose (in my case, 80mg/day, or 1mg/kg of body weight) as soon as the taper is completed.
Now, this taper thing is kind of tricky. Turns out that the body’s adrenal glands–in addition to cranking out adrenalin on request–manufacture approximately 5mg of their own “prednisone” in the form of cortisol, a similar glucocorticoid. Since this paltry 5mg dose is dwarfed by the 80mg I’ve been ingesting from last December through May of this year, and again from August through the present, my body, as would anyone’s, shut down its own internal cortisol production during that first steroid regimen, and closed up shop again this time around, reasoning that there’s little point in cranking out a meagre 5mg when the body is being flooded with 80mg each and every day.
That’s all well and fine, but if one were to abruptly halt the prednisone regimen–a tempting prospect given the myriad of side effects that accompany such a high dose–the adrenal glands are not capable of returning to their own steroid production levels without some advance notice; rather, they need to be eased into their pre-prednisone production levels gradually. Otherwise, the adrenals might never awaken, and therefore be incapable of producing their own cortisol as well as other stress response hormones.
In fact, the adrenals are at some risk of being permanently compromised whenever a whole bunch of steroids are introduced. Hence, the rationale for tapering even the briefest regimen of prednisone. For cGVHD patients and others who are on relatively massive doses, the taper typically takes place over the course of a few months–80mg/day to 70mg/day for a week or two, then 70mg to 60mg for a few more weeks, and so on until the dose is finally reduced to zero.
There is, however, another approach to this tapering process; namely, the alternate-day method, wherein the actual tapering begins much sooner than with the standard protocol, but instead of dropping from 80mg to 70mg every day, the dose decreases to 70mg every other day, and then moves fairly quickly down to 0mg on that alternate day only.
So when one arrives at the 80mg on day one/0mg on day two point, the dose is already tapered down to 40mg when you do the math. The side effects are potentially minimized as well, although I’m still waiting for my chipmunk cheeks and calcium-challenged spinal column to avail themselves of this alleged respite. In any case, this alternate day option seems like it could be a winner for those who dream of a corticosteroid-free existence. There is a potential downside to this method, of course, that being the “roller coaster” effect one is subject to when zig-zagging between 80mg and 0mg doses over the course of 24 hrs.
I lobbied my docs for the alternate-day taper this time around, and for me, while the ups and downs are certainly noticeable, I have not found them to be unmanageable. The 80mg days find me juiced up and somewhat manic, while the “zero days” are characterized by a relatively normal feeling in the AM, followed by what can best be described as “running out of gas” by the early afternoon. Next day, it’s back to 80mg in the AM and the cycle begins again.
For now, it’s worth it to have the opportunity to get off the prednisone as quickly as possible and to know that I’m already down to 40mg/day. Coincidentally enough, my first “zero day” was Tuesday, Dec. 3rd, which dovetails perfectly with this blog posting, because if you are inclined to do just a little more math you will discover that the twelfth zero day of my taper just happens to fall on Christmas Day.
So let’s bring this posting full circle by setting the taper to music. I’ll jump right to day twelve to save electrons–and also to give you more time to read my second post of the day. I’ve found this to be surprisingly melodic, but please, folks, don’t feel that you absolutely must sing it out loud–it works just as well if you hum the tune and just read the lyrics to yourself. On the other hand, if there are others present in the room while you are reading this, why not all join in and give it full voice?
The more perceptive viewers among you may feel compelled to point out that precisely six zero days are included in my hastily-revised lyrics, as opposed to the twelve promised by virtue of this post’s title. In my defense, I opted to employ a not-inconsiderable degree of artistic license in order to maintain your interest through the entire stanza.
And now, without further ado:
The Twelve Zero Days of Christmas (Day 12)
On the twelfth day of Christmas
My docs prescribed to me
A normal dose of eighty
Zero on the next day
Then right back to eighty
Followed up by zero
Once again, take eighty
Drop back down to zero
Eighty, then revert to
Zero
mil-
li-
grams…
Eighty milligrams
No milligrams
Eighty milligrams
And a whopping dose
Of zero milligrams
Next: The Gift of the Mac Guy


